In South-East Asia, 99% of children under 5 years live in environments with airborne fine particulate (PM2.5) concentrations above WHO guidelines, and the attributable death rate in this age group has risen to ~75 per 100,000 children [1]. The South-East Asian region also bears most of the burden of non-communicable diseases (NCDs) and deaths in adults related to particulate air pollution (PAP). In 2012, alone, there were 800,000 deaths [2]. Children exposed to PAP are predicted, throughout their life-course, to experience illness and neurodevelopmental issues with considerable risk to quality of life and earning potential. This limits the ability of their societies to function, develop sustainably, and prosper [3]. Reducing exposure to PAP is one of four actions identified in UNICEF’s frame-work for improving children’s health [4]. However, PAP is a pervasive hazard, present in both indoor and outdoor environments. Children must attend school, exercise and play, and their exposures may be higher than adults’, as they inhale more pollution per unit body weight and have less agency to enact their own lifestyle changes [5].
Whilst, rightly, many agencies are implementing and recommending collective and personal emissions reduction strategies as the primary intervention [6], until air quality reaches acceptable levels, policy makers must ‘face-up’ to the fact that communities in LMICs want some control, by implementing exposure reduction strategies, to protect themselves and their children, fuelled by myriad media articles offering advice [e.g. 7]. Yet, without evidence-based advice, these currently untested protective actions, to reduce inhalation of PAP, may lead to behaviours where exposure may even be increased.
Previous work undertaken by members of this consortium has amassed evidence of local societal concerns regarding the protection of children from PAP in Indonesia [8 and direct community feedback]. Yet these concerns are not limited to the local: increasing coverage in international media has recently cast the topic onto the global stage [e.g. 9,10] with abundant images of children wearing facemasks to reduce PAP exposure appearing in news articles and on agency websites. This is fuelled by a proliferation of companies producing respirator-grade (N95) facemasks for children and adults following the Covid-19 pandemic – with no evidence of efficacy beyond the quality of the materials – and by increasing access to low quality alternatives [7,8,11].
The FACE-UP consortium will take the position of urban dwellers in LMICs who want to be empowered to take protective actions against PAP. Through an interdisciplinary, challenge-led approach to the co-design, implementation and evaluation of contextually-viable ethical practices and interventions, we will provide the first evidence on the effectiveness of different practices, how sustainable they are for long-term use, how local context (at household and policy levels) will impact their availability, effectiveness and potential for uptake, and how uptake will influence a reduction in related NCDs. We will also enable evidence-based policies and recommendations for improved urban health and promotion of the UN’s Sustainable Development Goals (SDGs; e.g. goals 3.4, 3.9 and 11.6).
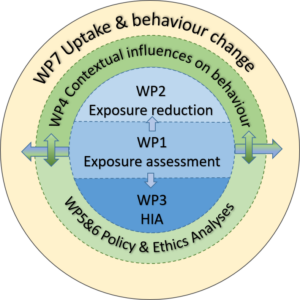
This project will develop and assess mechanisms to decrease children’s exposure to PAP in urban locations in two DAC-listed Asian countries: Indonesia and Nepal. Both suffer from severe PAP from vehicle, construction, industry and biomass burning sources, yet are home to different cultures, demographics, religions, socioeconomics, climates, built environments and policies. All of these contextual factors impact people’s potential for ill health, and their motivation, opportunity and capability to reduce exposure. The project has three overarching objectives (supported by subsidiary objectives), which inform an integrated, co-designed conceptual framework of research (Fig. 1). We will:
1) Establish context by assessing children’s exposure to PAP, identifying culturally-sensitive protective actions, assessing drivers that will influence behaviour change, and evaluating local learning behaviours;
2) Develop and test context-sensitive interventions to reduce children’s PAP exposures, including personal practices, and health impact assessment of their potential to reduce NCDs; 3) Promote sustainable behaviour change via assessments of ethical issues, policy requirements, logistics of access to intervention materials and co-development and evaluation of informational products to maximise their usefulness and uptake at a local and global level.
References
[1] WHO, 2018. [2] WHO, 2016 ISBN:9789241511353. [3] World Bank, 2016 #108141. [4] UNICEF, 2016 ISBN:9789280648546. [5] WHO, 2019. [6] Public Health England, 2019 #2018572. [7] Times of India, 2017, 2018. [8] Covey, Horwell, Rachmawati et al. 2019. Int. J. Disast. Risk Red. 35:101066. [9] National Geographic, Apr. 2019, Cities Issue. [10] The Guardian, 2014. [11] Horwell et al. 2017. J. Volcanol. Geotherm. Res. 382, 92-102.